
“Figuratively, I would say, the TBS, is the ‘devil’ our society cannot and will not do without because, there will always be persons who believe in them and must visit them first before reverting to the hospitals after being harmed. So here is my take on this:”

*Dr. Popoola Margaret Owoloyi MBBS, MPH
PEGASUS REPORTERS, LAGOS | FEBRUARY 5, 2022
Nazifi just graduated from secondary school. It was the most joyous event of his life. He never knew he could pull it but he did. When his friend Sadiq came in 30minutes later on his shiny new motorcycle popularly called ‘robaroba’, he knew they were going to paint the town red, and so they did. They rode recklessly through town and soon there was a ghastly accident that left Sadiq dead and Nazifi with multiple fractures.
He was rushed to the hospital where he received preliminary care to stabilize him. His parents however declined consent for further high level care because, they wanted Nazifi’s broken bones treated by the Traditional Bone Setter(TBS) in their home town. He was ‘renowned’ for tackling fractures such as Nazifi’s they said, and whisked him away to their trusted bone setter, as all well meaning entreaties fell on deaf ears.
Few years down the line, Nazifi was back in the orthopaedic clinic of the same hospital seeking medical intervention for his grotesquely mal-united (deformed) left lower limb.
Of course, the orthopaedic surgeons will restore his limb to the best of their ability and Nazifi and his parents will pay a handsome fee, but all of this could have been avoided at the beginning by not going to the traditional bone setter in the first place. Like Nazifi and his parents, many Nigerians fall into this category of people who believe all fractures must be treated at home by the TBS. Usually, not many are as lucky as Nazifi for making it out with a deformed limb. Many loose their limbs to amputations to salvage their lives while a few, lose their lives as a result of overwhelming infection.
WHAT EXACTLY IS A FRACTURE
A fracture is a break in the structural continuity of a bone.
EPIDEMIOLGY
According to available data, in Nigeria, road traffic accidents are responsible for 82.9% of the fractures that occur. Of this number, 64.3% of the cases are as a result of motorcycle accidents.
CAUSES OF FRACTURE
1. Trauma (High Energy Injuries)
a. Motor vehicular crashes from road traffic accidents.
b. Motor cycle accidents
c. Fall from height
d. Industrial accidents
e. Fueds/Machete cuts
f. Gunshot injuries etc
g. Tackle during a football match.
2. Low Energy injuries
a. Domestic falls
3. Some Systemic illnesses e.g Osteoporosis (common in elderly post menopausal women), Paget’s Disease, some Cancers, Chronic Osteomyelitis etc
4. Overuse: Repetitive motion can tire muscles and place more force on bone leading to fracture. Common among the forces eg The Military.
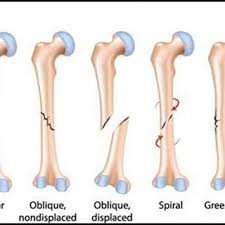
*Types of fracture
CLASSIFICATION
There are many ways to classify fractures however we will explore just a few.
1. Open or closed
2. Displaced or Undisplaced
3. Based on the pattern of the fracture, it can be:
a. Transverse
b. Oblique
c. Spiral
d. Greenstick
e. Impacted
f. Segmental
g. Comminuted
h. Stress
4.Pathological Fractures.
These are fractures that occur in diseased bones. They occur in bones of people with background medical conditions like Metastatic Cancers eg Breast Cancer, Multiple Myeloma, Osteosarcoma, other medical conditions like Sickle cell anaemia, Chronic Osteomyelitis etc
5. It can also be classified based on eponyms. That is named fractures. Eg. Smith’s fracture, Monteggia fracture, Colles fracture, Aviator’s fracture to mention but a few.
There are many named fractures and the description for each named fracture is universal such that Smith’s fracture in Nigeria, is Smith’s fracture world over.
WHAT HAPPENS WHEN A FRACTURE OCCURS?
When a fracture occurs, there is bleeding leading to what is called a heamatoma formation. Thereafter, some chemical agents are released to set in motion the fracture healing process. All of these follow some sequences referred to as stages of fracture healing viz a viz:
a. Hematoma formation (Day 1 – 5)
b. Fibrocartilagenous (Soft) callus formation (Day 5 – 11)
c. Bony(Hard) Callus formation (Day11 – 28)
d. Bone remodelling (Day 18 onwards. Can take months and years)
This shows that, the body has the potential to heal itself once there’s a broken bone, and this is true for most fractures except for some special ones that must be fixed surgically or would never heal. The tricky part however, is that the outcome of that ‘healing by itself’ may not be the desired outcome as it may heal in an abnormal position that may hinder full function, thereby leading to complications of fracture healing such as:
1. Mal – union ( when the fractured bone unites but in an abnormal position). This may give rise to:
a. Shortening of the affected limb
b. Angular deformities
2. Delayed union
3. Non – Union (when the fracture fails to unite for an extended period after the time which it should have united)
4. Nerve and vascular injuries
5. Premature physeal closure
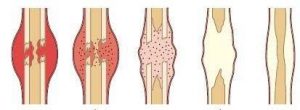
*Healing stages of a fractured bone
THE TBS BURDEN
The Traditional Bone Setter in Nigeria enjoys a huge patronage and the reason for this is not far fetched.
Where we come from, our religion and culture play strong roles in the decisions we take particularly concerning our health. In most of our communities, once fracture occurs, the first person to consult is usually the traditional bone setter. There have been times, when they’ve had good outcomes but overwhelmingly, they’ve had many disastrous outcomes that had to be salvaged by the orthopaedic surgeons in the hospitals. Why this happens is simple; the body has potential to heal itself most times, so all it needs its the right positioning and appropriate intervention as at when due.
The principles of fracture management are basically reduction (realign), immobilization (stabilize the fracture in the desired position) and rehabilitation. Now, while the orthopaedic surgeon has this knowledge and the technical know how to carry out his/her intervention, to achieve remarkable success, the traditional bone setter is ‘blind’. He has no knowledge of the science behind the mechanism of injury in a fracture, and neither does he have the knowledge of the biology of fracture healing. He may have some skills but has no technical aid or the ability to study, understand and use relevant aids (eg. xrays, CT Scans etc) even when such are available. He has no knowledge of how to reduce (realign) fracture appropriately or use splints safely in a way that will not compromise nerves and blood vessels.
He does not understand that making scarification with unsterilised blade is wrong. Neither does he know that applying unsafe concoctions to such scarification is dangerous. Most daunting of all is that he does not understand that he has no business treating open fractures at all, let alone treating them in septic conditions.
The burden is enormous, seeing that by default, the TBS who is ill equipped to take care of our fractures, have been made the ‘first on call’ by our society. It becomes even more dangerous when this ‘first on call’ is ‘blind’, seeing that he has no training or ability to use basic aids in effecting his trade.
WAY FORWARD
Figuratively, I would say, the TBS, is the ‘devil’ our society cannot and will not do without because, there will always be persons who believe in them and must visit them first before reverting to the hospitals after being harmed. So here is my take on this;
* We could take a survey of TBS across the nation.
* Document those who seem to be able to handle some basic things.
* Give them some basic trainings on how to know some simple cases that can be handled at home and those they MUST send to the hospital. As authority figures, if a patient goes to them and the patient does not fit the case descriptions of those he can treat at home, if he tells them to go to the hospital, they definitely will.
* Then, for the simple ones to be treated at home, they (TBS) can have some guide on what to do safely and when to call for help when things get out of hand.
* They can be taught on how to use basic splints safely and how to use basic aids to guide their work.
* The documented ones can have officers of health monitor their work to keep them in line.
* There’s a relationship such as this in Obstetrics and Gynaecology that is working out well. That is the training of TBA’s (Traditional Birth Attendants) in local communities.
If this relationship is explored in Orthopaedics, it might help in decreasing the huge amounts of TBS related complications the orthopaedic surgeon has to attend to.
CONCLUSION
In order to tackle the menace of the TBS and improve our health indices, we must think out of the box. If we take up the Obst & Gynae method of training TBA’s, and implement it in orthopaedic by training TBS’s, it might be one solution out of the many options to take, WHEN THE FIRST ON CALL IS ‘BLIND’.
REFERENCES
1. Maheshwari, Essentials of Orthopaedics
2. https://www.njotonline.org
3. https://www.ajol.info
2 Attachments

*Dr. Popoola Margaret O
Dr. Popoola Margaret Owoloyi MBBS, MPH also known as Dr. Meg, is an Orthopedic Surgeon in training at the Ahmadu Bello University Teaching Hospital, Zaria. She’s a Reverse Medical Tourism advocate and a champion of the call for a better health system for Nigeria and Nigerians. She is the ED, C-HELP Nigeria, Coordinator, Irawo Book club and the Chief Navigator at WOW Consult, a Patient Navigation outfit that seeks to connect patients to the appropriate health facility for their medical condition locally, thereby encouraging Reversal of Medical Tourism. She is the author of the financial bestseller NAIRA BOSS and the amazing medical text, EVERY PREGNANT WOMAN ( with Hausa translation) amongst others.
Dr. Popoola Margaret is the Convener of the C-HELP’s HEALTH SUMMIT and ANNUAL CANCER AWARENESS ROAD WALK. She is also the Convener of the HEROES of HEALTH AWARDS. JMBSR – a medical and basic science journal, is also floated by her organisation, C-HELP.
Notice: We Apologize for publishing this column late. Dr. Popoola’s column is still an every Friday publication… Editor
What’s your view? Tell us you were here by replying to this story in the comment section below. You can share it, too.
Pegasus Reporters: making news that reach your audience | Advertise with us!|Join our readers’ list on Telegram (+234 813 308 8344) Follow us on Twitter @pegasusreporters | We are on Facebook; The PegasusReporters | Chat with the Editor on WhatsApp (+234 815 444 5334) |Contact the Editor or send your articles to pegasusreporters@gmail.com
Read Our preceding Post: Political Arena: Shaka Momodu’s Jaundiced Viewpoint On Tinubu – Mr Tunde Rahman.
